
By J.E. Williams, OMD, FAAIM
Testing patients for C-Reactive Protein (CRP) is as necessary to disease prevention as flossing your teeth or getting your LDL cholesterol level checked. Because CRP is a key marker for inflammation, routine monitoring can help prevent cardiovascular disease and save lives.
C-Reactive Protein (CRP) is a type of protein secreted from the liver that increases in response to inflammation. It is particularly sensitive to inflammation in the walls of coronary arteries. CRP is present in the acute phase of infection or inflammation, as well as during chronic inflammation. High levels are diagnostic tip-offs for coronary artery disease, but also for diabetes or cancer. Patients with very high CRP are more prone to develop stroke, heart attack, and peripheral vascular disease. CRP is also high in cases of colitis and Crohn’s disease. Patients with autoimmune conditions like rheumatoid arthritis can also have high CRP.
What is the best CRP test?
There are two tests for C-Reactive Protein:
- CRP Quantitative is a marker in the blood that rises rapidly in response to injury and inflammation. High levels help detect hidden infections and useful for monitoring response to anti-inflammatory therapy. If therapy is successful, CRP level returns to normal. The standard reference range is 0.0 – 4.9 mg/L for LabCorp, and 0.0 – 0.8 mg/dL for Quest Diagnostics and ARUP Laboratories.
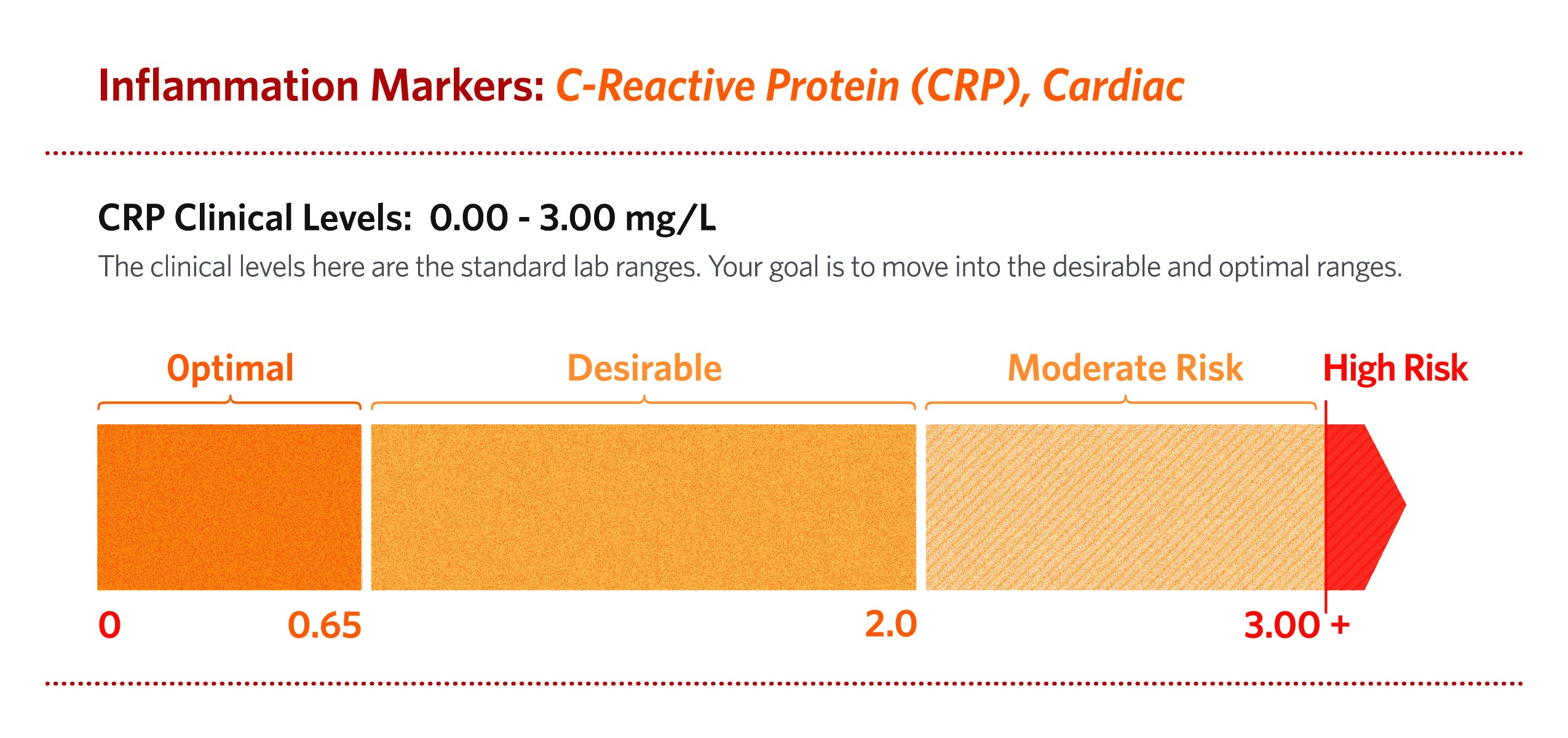
- CRP highly sensitive (hs-CRP), also termed CRP cardiac, predicts high-risk patients with cardiovascular and peripheral vascular disease. Inflammation plays a fundamental role in all phases of atherosclerosis. CRP actively participates in atherogenesis. (Salazar et al., 2014)The normal range for hs-CRP is 0.00 – 3.00 mg/L.
5 reasons to test hs-CRP
- Accurate marker of inflammation
- Targets inflammation in arteries
- Predicts cardiovascular and peripheral vascular disease risk
- Predicts cancer risk
- Predicts metabolic syndrome risk (Devaraj, Valleggi, Siegel, & Jialal, 2010)
- Predicts fatty liver disease (Lee et al., 2017)
The hs-CRP relavtive risk scale
Results for hs-CRP provide a scale of relative risk. Less than 1.00 is the best. Over 3.00 is considered very high risk. A level over 10.00 is associated with infection and acute inflammation, a marker for unusually high risk for cardiovascular disease.
Cardiovascular and metabolic risk factors tend to cluster. For example: total cholesterol and LDL may be moderately high, and HDL low. But, if hs-CRP is elevated, taken together the high hs-CRP magnifies the risk for a heart attack or stroke. (Ridker, 2005)
For a fasting blood sample, keep in mind that variations of hs-CRP occur during the course of the day. The highest levels occur in the morning and the lowest levels at midday. (Koc, Karaarslan, Abali, & Batur, 2010) For serial testing, advise patients to have their blood draw at the same time of day.
What is the optimal cut off point For hs-CRP?
Decades of research went into to the study of CRP, and it’s now widely accepted as a predictor of risk for cardiovascular disease and metabolic syndrome, itself a risk factor for heart disease. Most studies on CRP were compiled in North America and Western Europe. Both areas of the world with high incidences of obesity, heart disease, metabolic syndrome, and diabetes. CRP is often elevated in all of these conditions.
But what about areas of the world that have lower incidences of cardiovascular disease, like Japan? What about American patients who live a healthy lifestyle and eat a plant-based Asian style or Mediterranean diet? Do hs-CRP level varies according to race, gender, and diet?
A Japanese study found that a better cut off point for this patient group may be 0.65 mg/L instead of 1.00 mg/L. In another study of patients with metabolic syndrome, the optimal cut off point may be 0.45. (Oda & Kawai, 2009) These studies suggest that the lower the hs-CRP value, the better.
 J. E. Williams 2017 The Complete Blood Test Blueprint ©
J. E. Williams 2017 The Complete Blood Test Blueprint ©
Test for hs-CRP because levels can be high without any symptoms. A morning fasting test is recommended. If your patient’s hs-CRP level is high, start with lifestyle and dietary changes and retest in six months.
For the average population, the low-risk range of less than 1.0 is acceptable. But, I prefer a tighter range. For my patients, who are mostly proactive about their health and already eat a predominantly plant-based diet, I agree with the Japanese study: an optimal cut off point would be less than 0.65. (Oda et al., 2006) Optimally, a hs-CRP close to zero is best.
About the Author:
 J. E. Williams, OMD, FAAIM is a pioneer in the field of integrative and functional medicine, longevity, and quality of life.His experience ranges from medical acupuncture to traditional Chinese and Ayurvedic medicine, naturopathic medicine, bioregulatory medicine, functional medicine, advanced injection therapies, intravenous therapies, anti-aging medicine, and cell rejuvenation. He was a founding faculty member of Pacific College of Oriental Medicine, and has taught at the University of Miami Miller School of Medicine and NOVA Southwestern University. He is the author of more than six books and programs including Viral Immunity and the Complete Blood Test Blueprint. For more information: http://drjewilliams.com/
J. E. Williams, OMD, FAAIM is a pioneer in the field of integrative and functional medicine, longevity, and quality of life.His experience ranges from medical acupuncture to traditional Chinese and Ayurvedic medicine, naturopathic medicine, bioregulatory medicine, functional medicine, advanced injection therapies, intravenous therapies, anti-aging medicine, and cell rejuvenation. He was a founding faculty member of Pacific College of Oriental Medicine, and has taught at the University of Miami Miller School of Medicine and NOVA Southwestern University. He is the author of more than six books and programs including Viral Immunity and the Complete Blood Test Blueprint. For more information: http://drjewilliams.com/
Power2Practice makes it easier to create, save, order and reorder compounded pain relief formulations.
Watch this video to see how Power2Practice saves time and money, then schedule a demo to learn even more…

References:
Devaraj, S., Valleggi, S., Siegel, D., & Jialal, I. (2010). Role of C-reactive protein in contributing to increased cardiovascular risk in metabolic syndrome. Current Atherosclerosis Reports, 12(2), 110–118. http://doi.org/10.1007/s11883-010-0098-3
Koc, M., Karaarslan, O., Abali, G., & Batur, M. K. (2010). Variation in high-sensitivity C-reactive protein levels over 24 hours in patients with stable coronary artery disease. Texas Heart Institute Journal, 37(1), 42–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/20200626%5Cnhttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC2829811%5Cnevernote:///view/469804855/s16/d0602bb4-c62a-4a32-a3f3-5760008b04a3/d0602bb4-c62a-4a32-a3f3-5760008b04a3/
Lee, J., Yoon, K., Ryu, S., Chang, Y., Kim, H.-R., & Nakano, T. (2017). High-normal levels of hs-CRP predict the development of non-alcoholic fatty liver in healthy men. PLOS ONE, 12(2), e0172666. http://doi.org/10.1371/journal.pone.0172666
Oda, E., & Kawai, R. (2009). Tentative cut point of high-sensitivity C-reactive protein for a component of metabolic syndrome in Japanese. Circ J, 73(April), 755–9. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19225207
Oda, E., Oohara, K., Abe, A., Veeraveedu, P. T., Watanabe, K., Kato, K., & Aizawa, Y. (2006). The optimal cut-off point of C-reactive protein as an optional component of metabolic syndrome in Japan. Circulation Journal : Official Journal of the Japanese Circulation Society, 70(4), 384–388. http://doi.org/10.1253/circj.70.384
Ridker, P. M. (2005). C-reactive protein, inflammation, and cardiovascular disease: Clinical Update. Current Issues in Cardiology, 32(3), 384–386.
Salazar, J., Martínez, M. S., Chávez-Castillo, M., Núñez, V., Añez, R., Torres, Y., … Bermúdez, V. (2014). C-Reactive Protein: An In-Depth Look into Structure, Function, and Regulation. International Scholarly Research Notices, 2014, 1–11. http://doi.org/10.1155/2014/653045