
By Paul Savage, MD, FAARM, ABAARM – Founder and Chief Medical Officer | Power2Practice
If your practice is anything like mine, you see many woman who want to be in optimal health and are ready to partner with you and focus on an integrative approach. However, very few of my female patients spend much time thinking about cardiovascular health until I bring it up. Although we practitioners consider many of these facts common knowledge, the general population is still largely unaware that cardiovascular disease is the #1 cause of death for women in the United States. Here is a rundown of interesting facts related to cardiovascular disease that you may like to share with your patients.
The Truth About Cardiovascular Disease in Women
Overview:
- The lifetime risk of a woman’s developing CVD by age 50 is an estimated 39%.1
- More than 42 million women are currently living with some form of cardiovascular disease.2
- More than 8 million women have a history of heart attack and/or angina.2
- Five and a half million women will suffer angina.2
- More than 200,000 women die each year from heart attacks– five times as many women as breast cancer.2
- Almost two-thirds (64%) of women who die suddenly of coronary heart disease have no previous symptoms.2
- More than 159,000 women die each year of congestive heart failure, accounting for 56.3% of all heart failure deaths.2
- 35.3% of deaths in American of women over the age of 20, or more than 432,000, are caused by cardiovascular disease each year.2
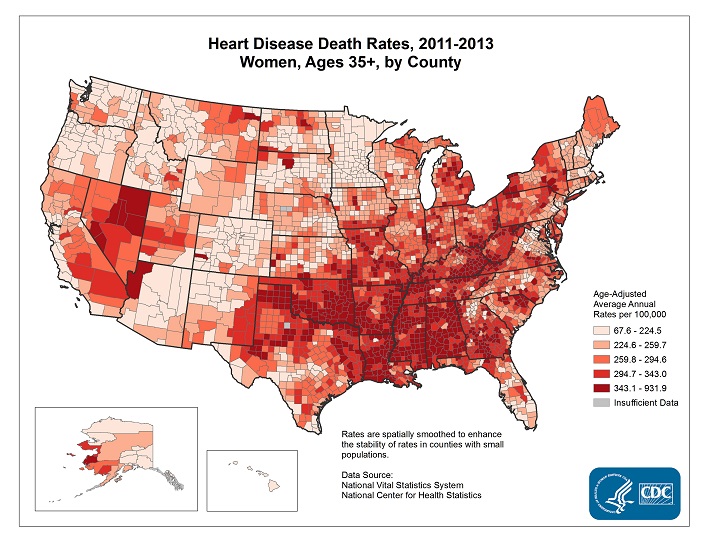
Also, take a look at this Interactive Atlas of Heart Disease and Stroke, where you may filter data by state, county and gender.
Risk Factors:
- 50% of women met neither aerobic activity nor muscle strengthening guidelines.3
- 14.8% of women 18 years and over smoke.3
- 16.4% of women reported binge alcohol use.3
- 67% of women 20 years and over are overweight or obese.3
- 38% of women 20 years and over are obese, specifically.3
- 33.4% of women 20 years have hypertension.3
Compared to Men:
- More women than men die of heart disease each year.3
- Men’s plaque distributes in clumps whereas women’s distributes more evenly throughout artery walls. This results in women’s angiographic studies being misinterpreted as “normal.”
- Women wait longer than men to go to an emergency room when having a heart attack and physicians are slower to recognize the presence of heart attacks in women because “characteristic” patterns of chest pain and EKG changes are less frequently present.
- After heart attack, women are less likely than men to receive beta blockers, ACE inhibitors and aspirin – therapies known to improve survival. This contributes to a higher rate of complications after heart attacks in women, even after adjusting for age.
- Women are almost twice as likely to have “Grade 3” obesity as men: 8.9% compared with 4.9%.3
- 23% of women (and 18% of men) will die within one year of a first recognized heart attack; 22-32% of women and 15-27% of men heart attack survivors will die within five years.
- 12-25% of women (and 7-22% of men) heart attack survivors will be diagnosed with heart failure within five years.
- Women’s hearts respond better than men’s to healthy lifestyle changes, yet only 2 percent of the NIH budget is dedicated to prevention.
- Women comprise only 27% of participants in all heart-related studies.2
In addition, some groups of women are more likely to develop cardiovascular disease than other groups:
- 56.9% of African American women and 45% of Hispanic women age 20 and over are obese, as compared to 36.2% of White women and 11.9% of Asian women.3
- 44% of African American women age 20 and over have hypertension, as compared to 28.6% of Hispanic women, 28% of White women and 25% of Asian women.3
- Hispanic women more frequently have biologic risk factors such as obesity and diabetes than do white women, but the rates of obesity and hypertension among Hispanic women are lower than in black women. Therefore, a greater magnitude of, earlier exposure to, and longer duration of hypertension in black women may contribute to their increased CVD mortality rate.5
- Older women have a greater chance of developing cardiovascular diseases than younger women, partly because the tendency to have heart-related problems increases with age.
- Older women, for example, are more likely to develop high blood pressure and high blood cholesterol levels, to be diabetic, to be overweight, and to exercise less than younger women. Also, after menopause, women are more apt to get cardiovascular diseases, in part because their bodies produce less estrogen.
- Women who have had early menopause, either naturally or by means of hysterectomy, are twice as likely to develop coronary heart disease as women of the same age who have not begun menopause.
Advanced Cardiometabolic Testing
Technology in the arena of heart disease has advanced substantially over the past 10 years. Thankfully we are now able to look well beyond the “Bad Cholesterol” myth! Studies prove that the concern is not the “Bad Cholesterol” but how the body produces, transports and retrieves the cholesterol. The number of LDL “bad” Cholesterol, the density of these particles and the apolipoproteins which guide these particles are much more important than the level (amount) of bad cholesterol which your body has.
I tend to look at the genetic code to determine the genetic predisposition to heart disease (Apolipoproteins) along with evaluating inflammation by the use of L-PLA, heart sensitive C-reactive protein, myeloperoxidase and fibrinogen values.
About the Author:

Dr. Paul Savage founded Power2Practice in 2011 and is currently serves as the Chief Medical Officer. He graduated from the University of Michigan Medical School in Emergency Medicine and later earned his board certification in Integrative Medicine at George Washington University.
Since 2004, he has practiced integrative medicine exclusively and is considered by many as one of the world’s foremost authorities in the area of integrative metabolic medicine (IMM), including bioidentical hormone therapy.
Dr. Savage is currently Founder and President of Chicago Integrative Care where he practices medicine. He continues to lecture worldwide and frequently provides expert insights on hormone therapy to major news media.
References & Online Sources:
- D’Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, Kannel WB. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation 2008;117(6):743–53. [PubMed]
- cardiosmart.org
- CDC US Health Report, 2015
- Coulter SA. Epidemiology of Cardiovascular Disease in Women: Risk, Advances, and Alarms. Coulter SA, ed. Texas Heart Institute Journal. 2011;38(2):145-147. [link]